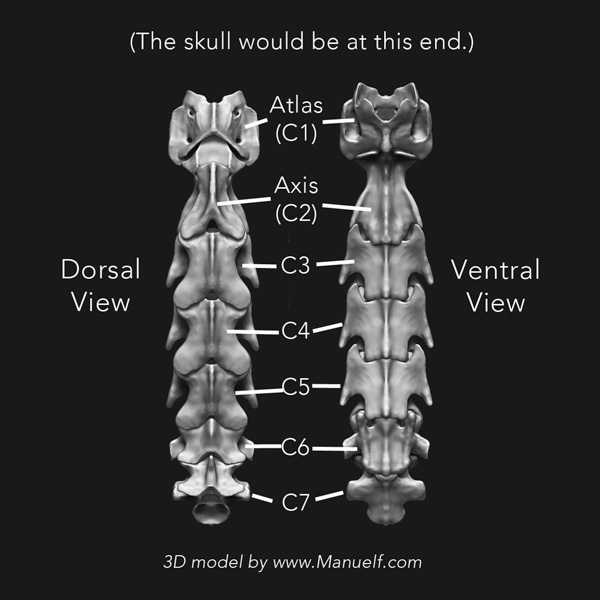
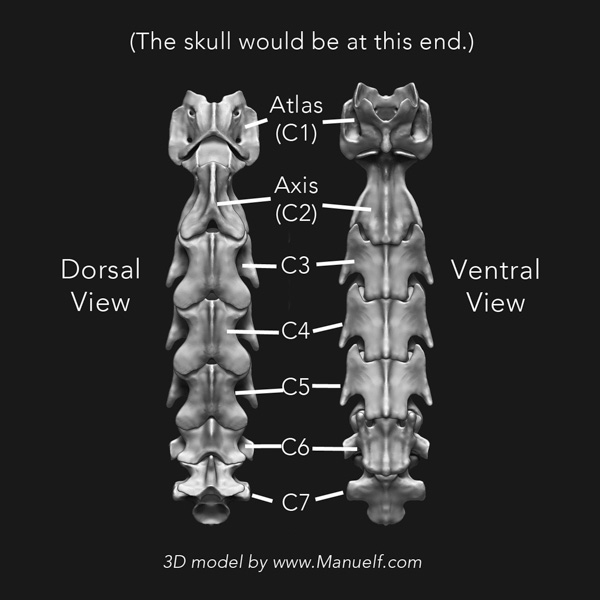
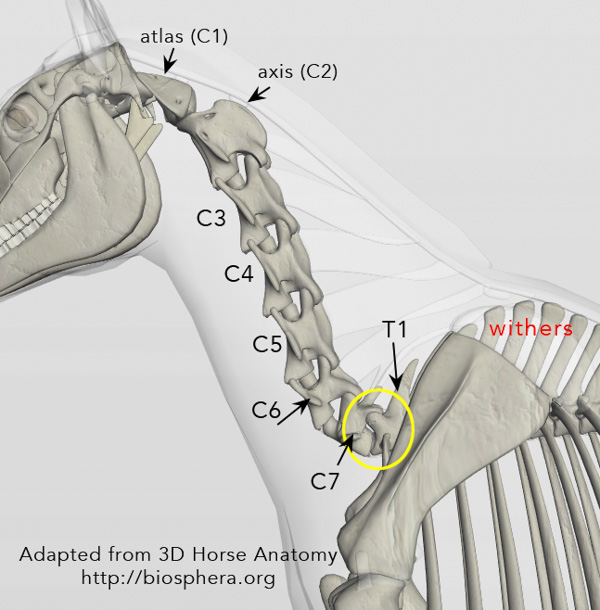
Seven vertebrae make up the neck portion of the horse's spine and are designated "C1 thru C7". C1, also known as the atlas, connects to the back of the skull at the atlantooccipital joint (poll).
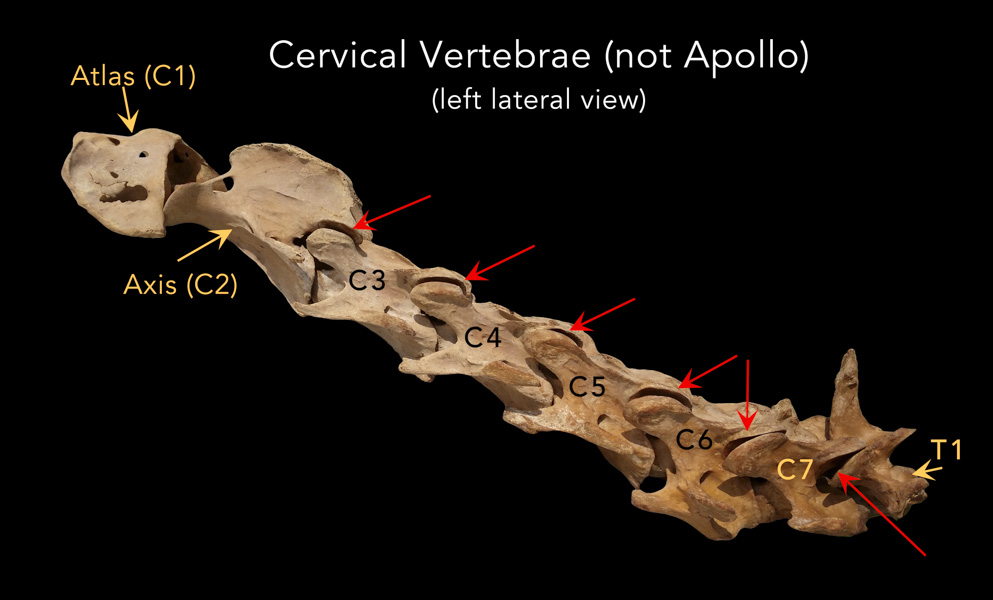
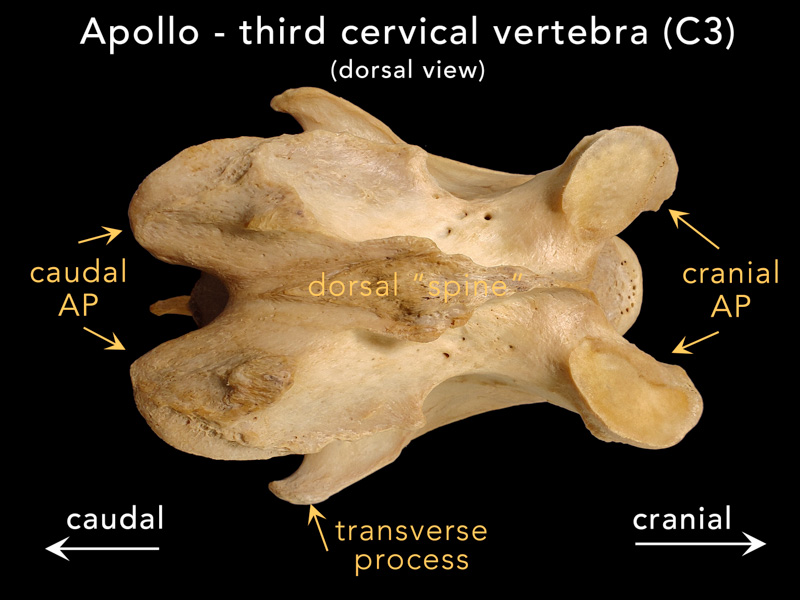
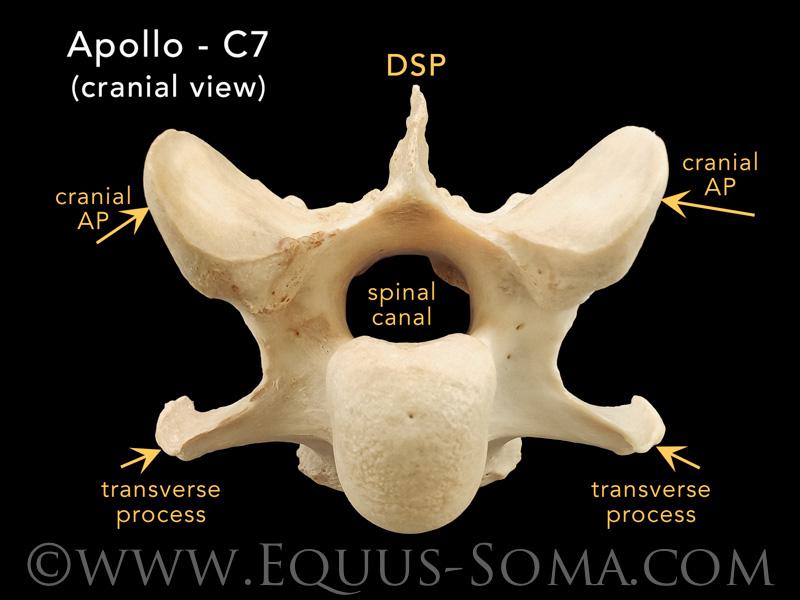
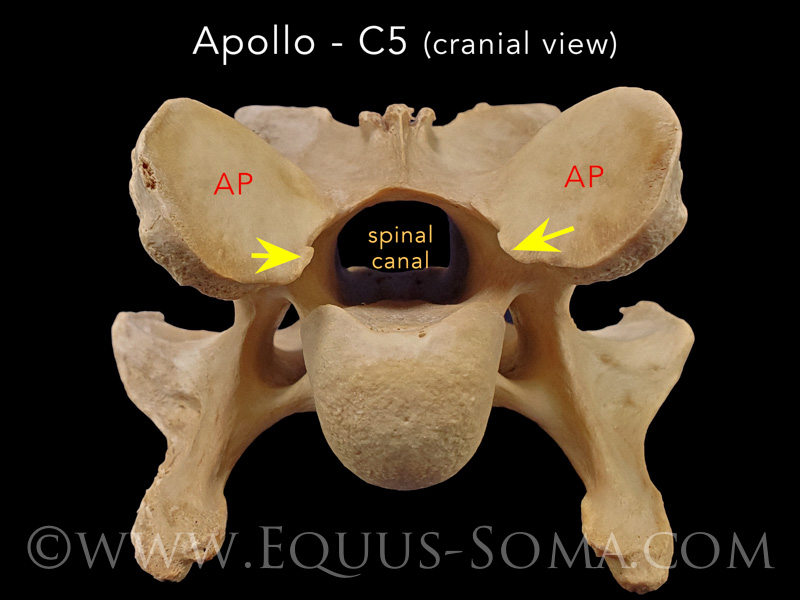
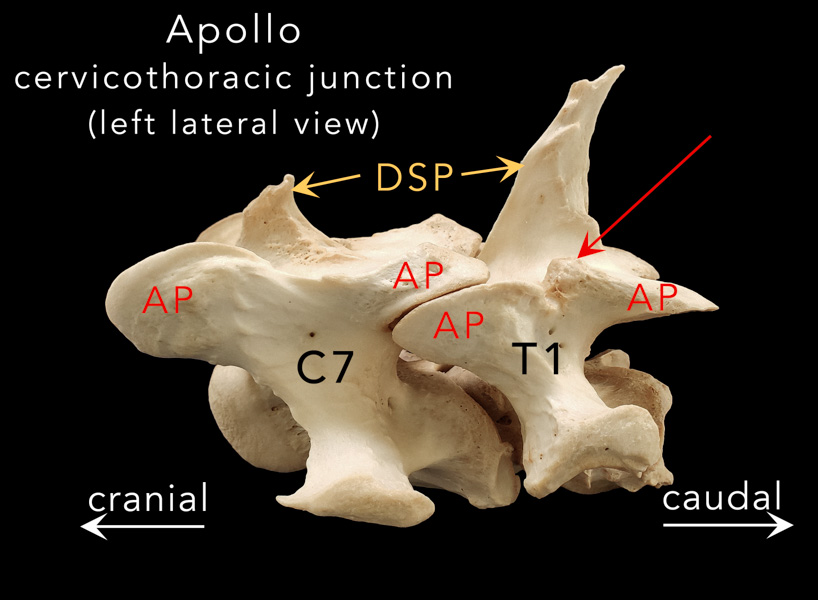
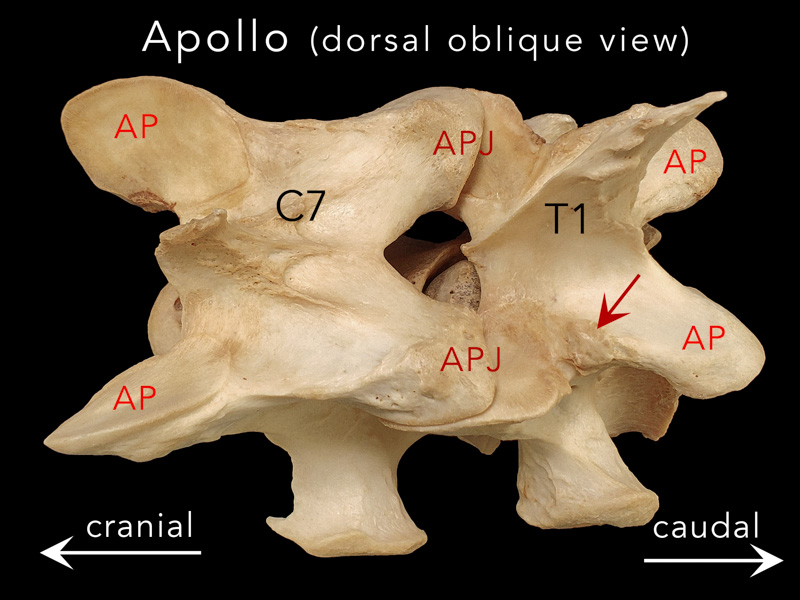
The atlas (C1) and its immediate caudal neighbor the axis (C2) each have unique morphology compared to the remaining cervical vertebra. C3, C4 and C5 are similar to each other. C6 has a pair of distinct long "ridges" or "tubercles" on the ventral surface. You can read more about C6 & C7 morphology (and their malformations) here.In the standing position there is an S-shaped curvature with a dorsal convexity at the poll and a ventral convexity at the C7-T1 junction.
Both junctions are regions of large ranges of motion in flexion and extension. (see Apollo refs #23 & 24)
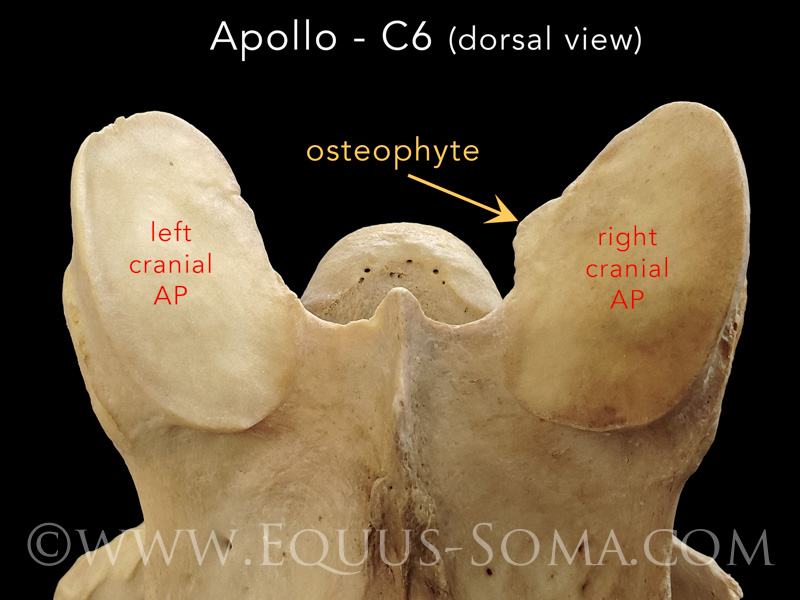
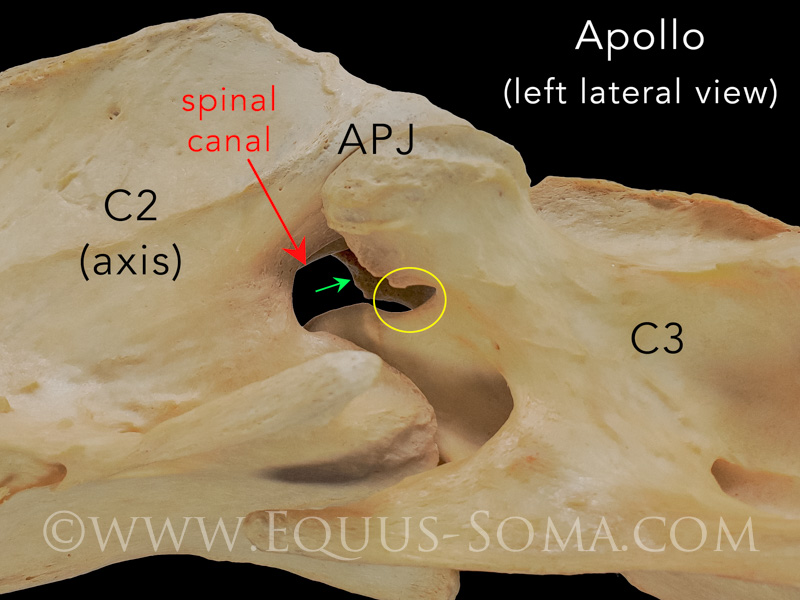
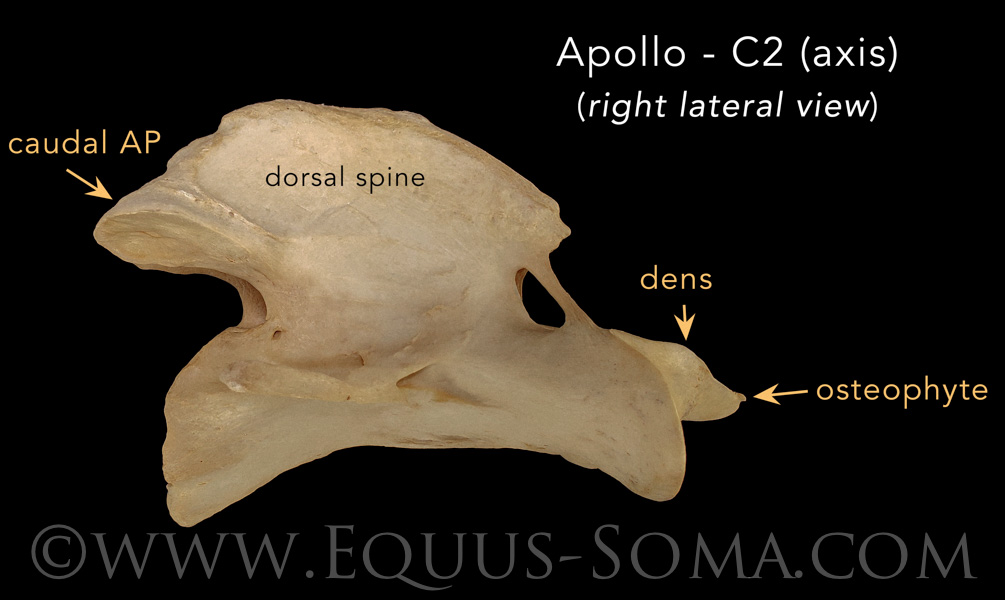
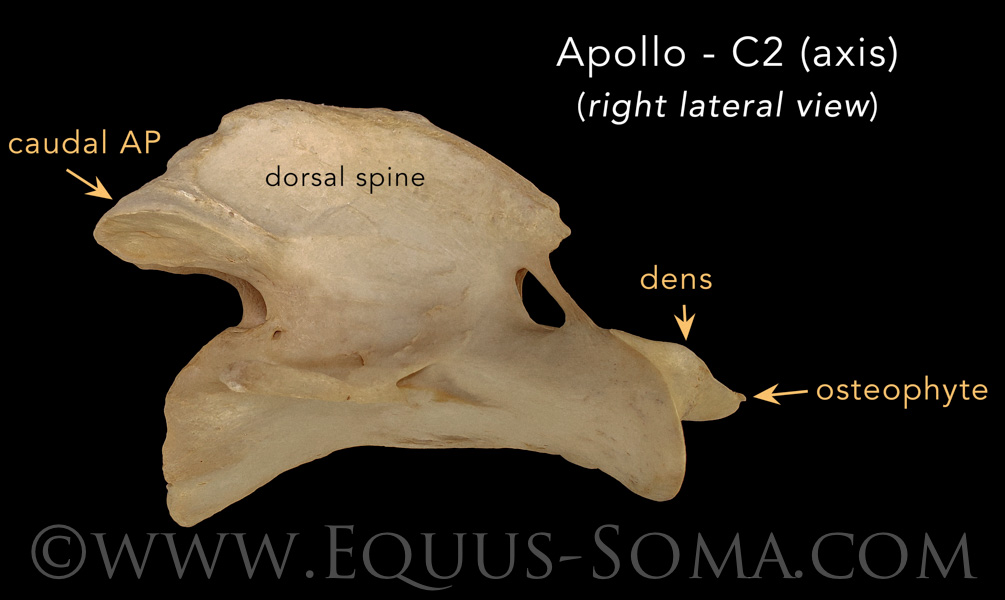
With respect to Apollo's second cervical vertebra (C2, a.k.a. "axis") the only obvious bony lesion is a small osteophyte on the right lateral edge of the dens, which we consider to be of "mild" grade.
On the other hand, Apollo's first cervical vertebra (C1, a.k.a. "atlas") presented with some very interesting lesions that we will elaborate on in Part Five where we describe his skull and the atlanto-occipital junction.